RE: UDI Requirements under an Emergency Use Authorization
By connect.raps.org
Published On :: Fri, 08 May 2020 00:25:42 -0400
From : Communities>>Regulatory Open Forum Bob, I stand corrected; if you confirmed with FDA that is good. From what I was reading and seeing (I must have missed that update) there was nothing addressing UDI or no UDI.for EUA products. (Personally I am a bit surprised at this since the whole concept of UDI is traceability and they waive this for emergency use products - when there is an issue this is where UDI becomes so important. Shrugs.) ------------------------------ Richard Vincins RAC Vice President Global Regulatory Affairs --- [More]
RE: UDI Requirements under an Emergency Use Authorization
By connect.raps.org
Published On :: Fri, 08 May 2020 05:33:11 -0400
From : Communities>>Regulatory Open Forum Hello Richard, Yesterday, I received a follow up from the Hotline (CDRH-EUA-Templates ) to my query. I was reminded that the waiver to good manufacturing practice and labeling requirements were included in the individual authorization letter. The person responding to my question concerning the UDI requirement provided the following: UDI is not specifically noted; however we are not enforcing UDI during the emergency. The specific authorization letter I was reviewing was for [More]
By polarisconsultants.blogspot.com
Published On :: Tue, 11 Oct 2016 07:06:00 +0000
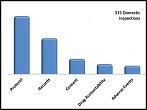
Year in and year out, protocol deviations are the most common FDA Site Inspection finding. Why does this keep happening?
If you’ve seen FDA’s Inspectional Observation Summaries, you know that in 2015 the most frequently cited violation in clinical research by far was “failure to conduct research in accordance with the investigational plan.” Do you know this finding also topped the list the year before that? And the year before that? In fact, deviating from the protocol has been the most common observation every year for the last decade.
Why does this keep happening?
The Nature of Protocols This will come as a surprise to no one: not all protocols are well written. Important procedures can be hidden in the most obscure places. Charts depicting Time and Events Schedules are famous for carrying dozens of footnotes that appear nowhere else in the protocol, yet convey important study procedures. For instance, a pre-dosing column may include a footnote that provides a timeframe for performing a physical exam; a post-dosing footnote might specify the interval at which vitals must be taken. Failing to follow study procedures compromises subject safety and data integrity; FDA won’t care whether the procedures were in big bold italics or 7-point font.
This, too, may come as no surprise, but not all protocols are error-free. Information in charts may not match the narrative. Procedures in Section A may conflict with procedures in Section B. When the FDA investigator spots an inconsistency, you’ll be asked which of the two conflicting procedures you followed and why. If you performed procedure A only because you didn’t even notice there was a B, it will be clear you didn’t read the protocol as thoroughly as you needed to. The FDA investigator may become concerned that your study execution differed from the sponsor’s intention. This is not a concern you want to trigger.
For these reasons, it’s imperative that study staff read and understand the protocol. Study team members need to ask questions about anything they’re unsure of, seek clarification on protocol inconsistencies, and get responses that satisfy before starting the study. A PowerPoint overview is not sufficient training.
One more irksome attribute of protocols that can make them difficult to follow -- they change. While most study sites allocate time and resources for initial protocol training, many lack a plan for training staff on protocol amendments. A disproportionate number of protocol deviations occur in amended procedures, and it’s often because staff members have been insufficiently trained on them. (And when you do train on protocol amendments, don’t forget to document it.)
Deviation Temptation A protocol is not a suggestion; PIs cannot substitute their own judgment for prescribed procedures, no matter how well-intentioned the departure. The protocol for a psoriasis study might call for the PI to perform a series of punch biopsies, very invasive procedures. After the first biopsy, an empathetic PI might be tempted to skip a second if he observes the plaque is clearing up; the drug is working. But this would be a protocol deviation. The protocol for another study might preclude the use of a particular drug, even though the drug is routinely used throughout the practice to treat a symptom that a study participant is exhibiting. But the study protocol trumps standard of care; prescribing the drug would be a protocol deviation.
A PI who feels she must deviate from the protocol for some reason must obtain prior approval, since failure to follow the protocol can jeopardize the reliability of the study data, if not subject rights and safety.
Deviations Happen So you’ve thoroughly read the protocol, you’ve asked your questions and received the necessary clarifications, you’ve trained your staff on the protocol and its amendments, and you do your best to follow them.
Despite all your preparation and vigilance, protocol deviations happen. They just do. And when they do, here are two don'ts.
(1) Don’t panic.
(2) Don’t let an FDA investigator find them first. Take the time to fully document any protocol deviations. Be sure to record why they happened, how they were corrected, and what was submitted to the IRB.
[Note: IRBs have different requirements about what types of protocol deviations should be communicated. Out-of-window visits are common and are frequently considered too minor to report. But nothing’s black and white. If the missed visit resulted in missed doses, that would probably change the calculus. The PI needs to determine whether to notify the IRB, and if no submission is thought necessary, it’s a good idea to document why not.]
By polarisconsultants.blogspot.com
Published On :: Mon, 19 Mar 2018 17:38:00 +0000
We may call them “site inspections”, but it’s not the site that’s being inspected when a regulator visits; it’s the Principal Investigator. Though a PI typically delegates study tasks to other staff members, he or she remains solely responsible for the conduct of the study. In fact, the ICH E6(R2) addendum adds two new sections to the international guidance that emphasize PI supervision.
That’s what makes the Delegation of Authority (DoA) log so important and why regulatory inspectors care about it so much. A DoA log serves as evidence that a PI has assigned study tasks only to those staff members with the education, training, and experience to carry them out. If delegates are unqualified to perform their tasks, subject safety could be at risk and it’s highly likely that the study data would be unusable.
Monitors – you can really make a big contribution here. At the outset of the study, you can verify that your PI has made appropriate delegations and the DoA log is complete. You can cross-match the log with training records, CVs, licenses, and source documents and correct any problems as early in the study as possible. Then, throughout the study, you can verify that the DoA log is being maintained.
Coverage Without referencing any other site document, monitors can spot two types of DoA log omissions.
(1) Missing Assignments. Are there study tasks to which no one has been delegated? The tasks in a DoA log are often represented by a short code to conserve space. A legend at the end of the log translates the code into its corresponding task. Monitors can compare the legend to the DoA log entries to see if any tasks are omitted.
(2) Gap in Assignments. Due to staff turnover, reassignment, leaves of absence, etc., delegation for a task frequently does not last the duration of the entire study. A column in the DoA log indicates the delegation start and stop date. Monitors can check to make sure that when the delegation for a task ends for one staff member, it is picked up by another.
Qualifications Once you’re satisfied the DoA log completely covers all tasks for the duration of the study, you can check to make sure delegates have the necessary qualifications. You’ll want to compare the log with training records, CVs, and medical licenses from the regulatory binder.
Has the staffer charged with recording vital signs during a subject visit been formally trained to take blood pressure? Is it documented?
Did an incoming pharmacist receive protocol training prior to the start date of his study assignments?
Does state law allow a registered nurse to dispense investigational product, or is a nurse practitioner or physician’s assistant required? Does the protocol require only an M.D. conduct certain procedures? Does the DoA log show the requirement is being followed?
Study Procedures Even after the focus of the monitoring visit moves past the DoA log itself, you should revisit the log during source document review.
Have any study tasks been conducted by staff members who have not received official delegation to do so?
Perhaps the protocol requires a blinded IP dispenser. If so, has the delegated dispenser conducted any other study procedure?
PI Oversight The PI is responsible for ensuring subject safety, compliance with the regs and the protocol, and control of the investigational product. That obligation cannot be delegated away. PI oversight is critical to a successful study, and the DoA log is where PI oversight starts.
Procedures that are performed by unqualified or ineligible personnel put both study participants and study data at risk. These are the very things regulatory inspectors work to guard against. Good monitors know it and make verifying the DoA log a priority.
__________________ A version of this article originally appeared in InSite, the Journal of the Society for Clinical Research Sites.
FDA approval delayed for Sanofi Genzyme’s next blockbuster
By www.bizjournals.com
Published On :: Fri, 28 Oct 2016 11:11:53 +0000
Editor's note: This story was originally published Friday morning, and has been updated to reflect the FDA's decision regarding the drug later that day.
A U.S. approval decision for a major drug planned to be marketed by Cambridge-based Sanofi Genzyme that had been expected last Friday has been delayed due to “deficiencies” found during a manufacturing site inspection in France.
In its third quarter report, released Friday morning, French drugmaker Sanofi (NYSE: SNY) disclosed that “manufacturing…
Sanofi and Regeneron provide update on U.S. Phase 2/3 adaptive-designed trial in hospitalized COVID-19 patients
By www.news.sanofi.us
Published On :: Mon, 27 Apr 2020 06:58:00 -0400
• Independent Data Monitoring Committee recommended continuing ongoing Phase 3 trial only in the more advanced “critical” group with Kevzara higher-dose versus placebo and discontinuing less advanced “severe” group
China publishes draft guideline for bevacizumab copy biologicals
By www.gabionline.net
Published On :: Fri, 08 May 2020 08:41:25 +0000
On 7 April 2020, China’s Center for Drug Evaluation (CDE) published draft guidance on clinical trials for the approval of bevacizumab copy biologicals. This guidance is the second specific guideline released by the CDE in April. The agency also released guidance on adalimumab on 1 April 2020 [1].
The COVID-19 Pandemic and Maintenance of a Continued Safe Food Supply
By strengthenfda.org
Published On :: Fri, 17 Apr 2020 18:38:51 +0000
The Alliance met (virtually) on April 15 with Dr. Caitlin Boon, FDA Associate Commissioner for Food Policy and Response and several of her colleagues. She described CFSAN’s and CVM’s role in responding to the current pandemic, as well as how the agency is assuring a continued safe food supply. About 50% of food spending in the […]
By strengthenfda.org
Published On :: Fri, 08 May 2020 19:30:32 +0000
Congress is starting to consider ways to address the budget cap problem that hangs over the entire FY 21 appropriations process for non-defense discretionary (NDD) programs. Last year, Congress broke a long-running stalemate by agreeing to budget caps for FY 20 and FY 21. They decided to front-load the increases, making spending decisions (relatively) easier […]
By childhoodcancer-mccaul.house.gov
Published On :: Wed, 23 May 2018 04:00:00 +0000
WASHINGTON, D.C. – Co-Chairs of the Childhood Cancer Caucus, Reps. Michael McCaul (R-TX), Jackie Speier (D-CA), Mike Kelly (R-PA), and G. K. Butterfield (D-NC), applaud the passage of the Senate companion to their bill – S. 292, the Childhood Cancer STAR Act.
The STAR Act passed the House today by a unanimous vote. It addresses the four major concerns facing the pediatric cancer community: Survivorship, Treatment, Access, and Research, and will elevate and prioritize the fight against childhood cancer at the National Institute of Health (NIH).
The members released the following joint statement:
"Today was a long anticipated day for the pediatric cancer community, and one to be celebrated. This bill is the most comprehensive childhood cancer bill to ever pass Congress and will finally head to the president’s desk to be signed into law. Childhood cancer remains one of the deadliest killers of our kids and we as a Congress, and a nation, must say, ‘Enough is enough.’ As co-chairs of the Childhood Cancer Caucus, we would like to thank all those who made this possible, including the Alliance for Childhood Cancer and theentire childhood cancer advocacy community.”
Click here to watch McCaul’s floor remarks ahead of the House passage of the STAR Act.
New Bipartisan ChiPACC Act Provides Better Medicaid Coverage to Children in Need
By childhoodcancer-mccaul.house.gov
Published On :: Fri, 27 Jul 2018 04:00:00 +0000
WASHINGTON, D.C. – Five lawmakers introduced a bipartisan bill giving a full range of medical services to families with children who have life-limiting illnesses and who qualify for Medicaid, which currently has gaps in such coverage.
The Children’s Program of All-Inclusive Coordinated Care (ChiPACC) Act (H.R. 6560) would let states create comprehensive care programs for these children. Its authors are the Co-Chairs of the Congressional Childhood Cancer Caucus: Representatives Michael McCaul (R-TX), Jackie Speier (D-CA), G.K.Butterfield (D-NC), and MikeKelly (R-PA), together with Representative Diana DeGette (D-CO), a senior member of the House Energy and Commerce Committee.
“Families with children facing life-limiting illnesses need all the support they can get, and they should be empowered to seek out that support,” the bill’s sponsors said in a joint statement. “We owe it to these kids and their loved ones to help ensure more compassionate care in their most trying times.”
Gaps in Medicaid coverage of hospice and palliative services have deprived many beneficiaries of the care they need because the program does not cover some of children’s unique medical needs.
Under this bill, the family of every child who qualifies for Medicaid will receive a specialized care plan covering a range of services – palliative, counseling, respite, expressive therapy and bereavement – providing them and their families greater comfort and peace of mind.
FDA Guidance on Clinical Trials During COVID-19 Pandemic
By eyeonfda.com
Published On :: Fri, 20 Mar 2020 12:34:27 +0000
Much attention has been paid to the impact of the COVID-19 pandemic on the supply chain for medicines we rely on, but there has been less focus on the impact of medicines yet to come. The advancements in cancer care … Continue reading →
T-Minus COVID-19 – Impact of Pandemic on New Medicine Launches
By eyeonfda.com
Published On :: Wed, 15 Apr 2020 11:51:47 +0000
As the coronavirus pandemic began to unfold, focus on the pharmaceutical and biotech sectors was on the most immediate and apparent concerns – the impact on the supply chain for drugs that are currently in the market and on the … Continue reading →
Impact of COVID-19 on FDA Enforcement and Approvals – Part 5 – FDA Provides Update to Shape Expectations on New Approvals
By eyeonfda.com
Published On :: Fri, 17 Apr 2020 15:45:55 +0000
In response to written questions submitted last month regarding the potential for delays, FDA had stated that “CDER remains fully capable to continue daily activities, while responding to the public needs of the current COVID-19 outbreak.” In a subsequent blog … Continue reading →
The Pharmaceutical-Biotech-Devices Industries Face a New World Post-Pandemic
By eyeonfda.com
Published On :: Mon, 04 May 2020 11:23:30 +0000
There is going to be a time in the not too distant future, when the fuller picture of the healthcare impacts of COVID-19 come into sharper focus. When that happens, it is not likely to be pretty. In large part, … Continue reading →
Indian manufacturers still deny drug quality problems and use same old rebuttals
By searchingforsafety.net
Published On :: Tue, 16 Sep 2014 11:25:27 GMT
Posted by Roger Bate The Economic Times of India covered our new paper today (see here). The paper published by the National bureau of Economic Research and not AEI as claimed by the Economic Times (see here), shows that Indian firms send their worst quality medicines to Africa. It is a shame that Indian Industry hack DG Shah continues to trot out the same arguments attacking us rather than addressing the paper’s findings. For example, he asks why did it take so long to publish a study [...]
ProPublica is a nonprofit newsroom that investigates abuses of power. Sign up to receive our biggest stories as soon as they’re published.
They’ve gotten to know New York City in a way many have not, through the low-wage work of cleaning its skyscrapers, serving its restaurants and crisscrossing its streets on bicycles, through long subway rides very early in the morning and very late at night. The saying goes: You’re not a true New Yorker unless you’ve lived here for a decade. They’ve done their time and felt a deep sense of belonging in this city of immigrants.
But, in the epicenter of a pandemic, the undocumented have never felt more alone.
They are losing loved ones but do not qualify for city funding to help bury them. They are getting sick but hesitating to get tested or go to the hospital, balancing their fear of the virus with their fear of exposure to immigration authorities. They are worried about supporting their families abroad as well as those who live with them, weighing whether to keep working perilous jobs or to stay home and somehow keep food on the table.
They’ve experienced separation, but not like this — out in the world, in a skeleton crew, wearing a mask to deliver food to closed doors; in cramped apartments, sectioned off, in an attempt to quarantine. They are divided across national borders as family members die, praying novenas on Google Hangouts. Their bodies cannot be buried, intact, where they were born; they move from hospital bed, to refrigerated truck, to incinerator.
ProPublica interviewed two dozen undocumented Latino immigrants and their families about their experiences with death, illness and survival. Some spoke on the condition of anonymity, afraid of being targeted. Others allowed us to use their first names or the full names of their family members who died.
One kitchen worker from the Bronx worked in the World Trade Center two decades ago. “We used to fill the back elevators of those towers,” he said. He lost friends on Sept. 11, 2001, who were not identified or acknowledged among the dead because their names did not match those on record or their families were unable to claim the bodies.
He and others spoke to ProPublica because this time they wanted their experiences to be counted as part of the story of their city, overtaken by a virus.
Barriers to a Proper Burial
Adrian Hernandez Lopez, 38, never planned to stay in New York City. His 15 year stint here was dotted with visits to his family in Mexico, for the baptism of his son, who is now almost a teen, and to check on the house he had been sending his paychecks to build.
For much of his life in New York, Adrian Hernandez Lopez worked in kitchens. “He got along with everyone, the manager loved him, he was a good worker,” his brother said.
(Courtesy of the Hernandez Lopez Family)
He and brother worked at an Italian restaurant in Times Square. “We were always together,” his brother said. They crossed the border together and, years later, commuted together from Queens to midtown Manhattan.
The last time they spoke by phone, Lopez waited in agony in a hard chair at Elmhurst Hospital, breathing in oxygen from a machine. He was transferred to Woodhull Hospital in Brooklyn. One day later, the father of two wound up in a vegetative state.
He died on April 2. His mother, who lives in Allende, a small village in the state of Puebla, wants him buried there, alongside two babies she lost just after birth.
He can’t be traditionally buried, despite the strong Mexican custom. More than 400 Mexican migrants are known to have died of COVID-19 in the New York area, but for health reasons, Mexico will only accept their bodies if they are cremated.
In place of seeing the body one last time, Lopez’s brother was sent photos by the funeral home, which will hold the cremains while the family figures out how to get them to Mexico.
The Mexican Consulate pledged financial aid to the families of nationals who died of COVID-19 complications, but it has been slow to materialize. According to Lopez’s brother, they’ve been asked to follow guidelines to receive a reimbursement. The Consulate General’s office in New York said it was not authorized by the Mexican government to give interviews at the time of our request for comment.
The city of New York provides burial assistance, but it requires a Social Security number for both the deceased and the person requesting funds. City officials say they are limited by federal and state law in the help they can offer. “We are exploring every possible option to ensure that all New Yorkers, regardless of immigration status, are able to bury their loved ones in the way they feel is most fitting,” city spokesperson Avery Cohen said.
Two members of the City Council have called for an emergency fund to provide assistance to all low-income families, including the undocumented.
“One of the most devastating calls I’m regularly getting is from people who can’t afford to bury their loved ones and aren’t eligible for any assistance,” Council Member Francisco Moya said in a release. “That’s simply not acceptable.”
Lopez’s family is one of several raising money for the transport and burial of their loved one who died in the United States.
As he tries to figure out how to send Lopez home, his brother sits in the small apartment they shared in Queens, with his wife and 6-year-old daughter, listening to the sirens that have become a constant reminder of their loss. He and his wife have been out of work for a month. They don’t know how they will pay the rent.
Deterred From Seeking Care
More than a dozen undocumented people told ProPublica that when they got sick, they stayed home, deterred from seeking care by the worry that they would not get it if they tried. They faced the same obstacles as everyone else in New York, where hospitals were crowded and unsafe, and feared additional ones involving their immigration status.
Fani lives in East Harlem. Over the last 18 years, she’s worked at a laundromat and a factory, a restaurant and as a babysitter. When she and her husband got sick they called 311. She said the voice on the other end confirmed their COVID-19 symptoms and told them to stay home unless they couldn’t breathe.
“They said there were no beds, no respirators. We healed each other as best we could with soups, teas and Tylenol,” she said.
Sonia, who became ill with COVID-19 symptoms almost three weeks ago, was afraid to go to the hospital. “I knew several people who went into the hospital with symptoms and they never came back,” she said. “That was my fear and why I decided to not go in. I preferred to isolate myself at home, with a lot of home remedies and hot teas.”
Multiple people said they knew hospitals had limited resources and worried they would be placed last in line for care because they were undocumented. “They’re going to let us die,” one man told his brother. A woman named Yogi in the Bronx said, “It might not be that they don’t want to treat us, maybe there weren’t enough supplies.”
Stories rippled through the Latino community about those who had difficulty getting care and those who could not be saved. According to a recent poll of voters in New York City, more than half of Latinos there said they know someone who died, the highest percentage of any group asked.
They hear stories about people like Juan Leonardo Torres, a 65-year-old retired doorman who knew someone on every corner of Corona, Queens. Unlike the others, Torres, from the Dominican Republic, was a citizen. Even so, he grew discouraged when he tried to get care.
Juan Leonardo Torres in 2016 with his newborn son, Dylan, at the same hospital where he would later seek COVID-19 care.
(Courtesy of the Torres family)
Within one week at the end of March, Torres had gone from feeling slightly ill to experiencing difficulty breathing and fevers that his wife Mindy tried to manage using herbs and other “remedios caseros,” or home remedies. She and her five sons who lived with them finally persuaded him to go to Long Island Jewish Medical Center Forest Hills, just a five-minute drive from the house.
When Torres arrived, he told his family there were not enough seats in the crowded emergency room. He gave his chair up to an older woman and stood for hours as staff connected and disconnected him to an oxygen tank.
Fifteen hours later, on a drizzly night, Torres appeared at the door of the family home. It was 2:30 a.m. He had made the walk alone and declared in Spanish, “For no reason do I want to go to the hospital to die like a dog.”
He spent the next three days quarantined in his son’s room, where he died.
As the family waited six hours for his body to be retrieved, his wife sat in the living room “like a statue.”
Calculating Survival
Unable to qualify for relief programs like unemployment and stimulus cash, undocumented people are faced with the difficult choice of working dangerous jobs or running out of the money they need for essentials like food and housing.
“The little we have goes to food,” said Berenice, who suffers from kidney problems and whose son struggles with asthma. She’s been home for weeks along with her husband Luis, who before the pandemic worked at a cab company.
“Yes, we need money, but there is also our health,” Berenice said. “We have family who are sick and friends who died. We are trying to survive.”
Luis has lived in New York for 18 years, working his way up from delivering pizza on a bicycle to owning a cab. He worries about exposing his wife and son. “I just want this to pass and we’ll see about starting over again,” he said.
Adan lives in the Bronx with his two teenage sons, who were born in New York City, and his wife. She cleaned homes. He worked in a restaurant in East Harlem. Neither are working and both overcame COVID-19. “The little money we had went to pay last month’s rent,” he said. “I don’t know what to do, we just want to work.”
He said his landlord always comes looking for the rent in person. He told “el señor” that he’s spending all his money on food. The man gave him flyers about unemployment, but Adan knows he won’t qualify. “Me las voy a ver duras,” he said. He’s going to see hard times. He said he has lived in the same building for 11 years and has never missed a payment. Even though he can’t be evicted now, he said, “the debt will be there.”
Adding to the pressure, for some, is that they also work to support family members in their home countries, who count on the money they send.
One delivery worker in Queens sends $400 to Mexico every two weeks to help his son, who studies biomedicine at a university in Puebla; that helps him cover what he needs for school, including rent and transportation. He sends another $300 each month to his elderly mother.
He said he remains one of only a few bicycle delivery workers at his diner who are still on the job, and he is seeing more orders than usual. He’s always worked six days a week, but this past month was so busy, he couldn’t stop to eat lunch or take breaks.
He would much rather be outside than at home, but the streets feel tense. “I feel strange not seeing anyone or saying hi anymore, but I think it’s much better this way,” he said. “I understand why people are afraid.”
Even though he doesn’t see them in the buildings he visits, customers have been conscious about leaving tips in envelopes. He feels grateful as he passes the long lines in Queens of those waiting for free food. It makes him sad to know how many need it now.
He rents a room in an apartment he shares with three other men who have all lost their jobs. One was in construction, the other two in restaurants. He takes precautions to keep them safe when he comes home, including changing his clothes before coming in. “It would be irresponsible not to,” he said.
He hopes the rules of social distancing, and his mask and gloves, will protect him. “I’m not scared,” he said. “If you are afraid all the time, you will get sick faster.”
ProPublica is a nonprofit newsroom that investigates abuses of power. Sign up to receive our biggest stories as soon as they’re published.
Last September, over pancakes at a diner in central Massachusetts, Molly Baldwin told her husband, Jonathan, they were going to have a baby. He cried into his coffee mug, elated and a little surprised. They had only been trying for about a week, and they had yearned for a summer baby, ideally in June, which would enable their parents to spend more time with their first grandchild.
“We thought we had the best timing,” she said.
But as the novel coronavirus began to spread through the country this year, Baldwin realized in early March that it was only a matter of time before the virus hit her town, Fitchburg, and the nursing home where she’s a social worker. Her patients would be among the most vulnerable: Some had battled addiction, many had experienced homelessness and most were elderly. Flu seasons were always hard on her patients, and she dreaded the havoc a more lethal disease would wreak.
Baldwin also worried about her baby. She spent hours looking up the prenatal effects of COVID-19, and the lack of evidence-based research concerned her. She called her obstetrician, who cautioned that because of the unknowns, she should consider working from home to limit her exposure to the virus.
So Baldwin made a plan for when COVID-19 arrived at her nursing home: She would swap shifts with a colleague to work fewer hours and request to work from home, as many of her duties are paperwork or computer-based.
She would work from the comfort of her kitchen table. She would avoid catching the virus. She would keep visiting her doctor until it was time to deliver, her belly swelling with a baby girl she knew was healthy and safe.
None of it, not a single thing, would go according to plan.
Baldwin said her supervisor and the human resources representative from the facility verbally agreed in mid-March to let her work from home. (Baldwin spoke with ProPublica on the condition that her workplace not be named; ProPublica contacted her employers with questions for this story.)
Then, on April 16, one of the residents at her facility tested positive for the virus. Baldwin sought testing at a walk-in clinic, and the results came back negative. But when she called her obstetrician’s office, she got a warning: If she continued to work at the facility, potentially exposing herself to the virus, they would not allow her to enter their office for prenatal appointments unless she could prove with a test, before each visit, that she was negative for COVID-19.
She understood their caution; her job was beginning to feel at odds with her pregnancy. It was time for her work-from-home plan to go into action.
She called her employer and asked to start the accommodations she had requested the month before. But they told her that now the plan would not be feasible, she said. Other pregnant employees were continuing to work at the facilities, and she would have to as well, she said she was told.
“The services provided at a nursing home do not typically allow for remote working,” a company spokesperson told ProPublica. “However, we have made changes to accommodate our staff whenever possible, provided there is no impact on patient care.”
After finding out her request to work from home would not be granted, Baldwin panicked. “I’m not even a mom yet,” she said. “This is my first baby, and I already feel like I’m doing everything wrong.”
Baldwin is one of dozens of pregnant workers who ProPublica has heard from who are navigating the risks of COVID-19 while in the field of health care.
“There are plenty of pregnant women across the country who are trying to figure out what to do to protect themselves, given the uncertainty,” said Emily Martin, vice president for education and workplace justice at the National Women’s Law Center. “If you feel like you can’t do your job because there aren’t certain accommodations and you feel like you’re at risk, it’s difficult to see where to go next.”
About half of the states have laws that allow pregnant women to request reasonable accommodations, including Massachusetts, Martin said.
According to the Massachusetts Pregnant Workers Fairness Act, signed into state law in July 2017, employers must grant reasonable accommodations to their pregnant employees that allow them to continue to do their job, “unless doing so would impose an ’undue hardship’ on the employer.” An employer also “cannot make an employee accept a particular accommodation if another reasonable accommodation would allow the employee to perform the essential functions of the job.”
Both the Centers for Disease Control and Prevention and the American College of Obstetricians and Gynecologists havestated that based on the data available, pregnant women do not face a higher risk of infection or severe morbidity related to COVID-19. That said, both the CDC and ACOG have suggested that health care facilities may want to consider reducing the exposure of pregnant health care workers to patients with confirmed or suspected COVID-19, if staffing permits.
“In the overwhelming majority of pregnancies, the person who is pregnant recovered well with mild illness,” said Dr. Neel Shah, an obstetrician and assistant professor at Harvard Medical School, echoing the current guidance. But, he cautioned, there is a lot we still don’t know about how the virus impacts bodies, let alone those that are pregnant. “We can’t say that it’s completely safe — we don’t know.”
Baldwin and her husband went through their options.
She couldn’t quit because they needed her paycheck. They had a mortgage, student loans and a new baby on the way. She also loved her job and cared deeply for her patients, whom she wanted to continue to serve. Her employer, trying to manage understaffing, had discouraged employees from taking time off, she said. She didn’t want to take any additional sick days, because she needed to save them for her maternity leave.
They decided that she would have to return to work.
Her employer told her to wear a mask and gloves, use hand sanitizer and remain in her small, boxy office, which has three desks for four people. Though she didn’t have contact with the residents, her office mates still did.
Baldwin’s job began to feel at odds with her pregnancy.
(Kayana Szymczak for ProPublica)
Even though she was scared, she tried to stay optimistic. “I was grateful for what I had because I have friends that are out of work right now,” she said. But she remained perplexed about why her requests had been denied. “I was sitting in my office doing work that would have easily been done from a laptop on my kitchen table.”
The company spokesperson did not respond to a question about whether it had originally given Baldwin verbal approval to work from home. When asked why she couldn’t have done the same work remotely, he said, “Based on your questions, our HR and Risk Management are anticipating action and would prefer to not comment at all.”
The next day, the Massachusetts National Guard delivered testing kits to the nursing home, and every resident was checked for the virus. When the results came back, at least 22 residents and 20 other staff members tested positive.
“We are conducting cleanings and infection control measures multiple times per day, with extra focus on high touch areas,” the company spokesperson said. “We screen and take the temperature of anyone entering our building, and we have increased monitoring of our residents.”
Public data shows the facility has more than 30 cases among residents and staff, the maximum number that the state reports publicly.
“I thought if I just keep working, stay in my office, use hand sanitizer, wear my mask, go home and shower right away, disinfect my clothes, then I will be fine, and I can keep my baby safe, and I can shed all this guilt,” she said.
Then on April 24, two of her office mates texted to tell her they had the virus.
And that morning, she’d felt a tickle in her throat.
“I know I’m positive,” she thought to herself, as she left work midday and drove to a CVS drugstore testing site an hour away that was offering free rapid tests for front-line and health care workers. Hundreds of cars were already lined up.
She waited alone in her Jeep Wrangler for three hours, wearing her mask as required, which muffled her nagging cough. She shifted around constantly, to keep blood from pooling in her swelling feet. At the front of the line, she received a 6-inch cotton swab, wedged it deep in her nasal cavity, and returned it to the technicians. They directed her into a side parking lot, and 30 minutes later, she got a phone call with her results.
“We’re sorry to tell you that you’re positive,” the voice on the line told her. Baldwin’s mind stalled, engulfed in a wave of anxiety, which gave way to seething frustration.
“This was so preventable,” she said. “Now here I am, 33 weeks pregnant and positive. My most important job is to keep the baby safe, and my actual job wasn’t making that happen.”
When she called her co-workers and supervisor to tell them she tested positive, she said they were “all very caring and compassionate.” They told her to stay home for at least a week, or until her symptoms subsided. The Families First Coronavirus Response Act requires most employers to provide their workers with two weeks of paid leave if the employee is quarantined or experiencing COVID-19 symptoms. Baldwin said she would have to exhaust her sick days first; she’d been saving them for her maternity leave. Her husband, who works as a correctional officer at a county jail, was allowed to take 14 days of paid leave to tend to his wife, without using his own sick days.
She could no longer go to her normal obstetrician for in-person appointments, and instead, she would have to rely on telemedicine. Her doctor connected her with an obstetrician specializing in COVID-19 cases, with whom she planned to meet this week.
Last Saturday, Baldwin’s mother had planned to throw her daughter a baby shower. She had invited 50 of their closest friends to celebrate at a new restaurant and had ordered dozens of pink favors from Etsy.
Because of the stay-at-home order, her shower morphed into a drive-by celebration, where her friends and family passed by her house, honking their horns and holding celebratory signs, balloons and streamers. They dropped gifts in front of her house, including first aid kits and a handsewn pink mask for an infant.
Her symptoms have, so far, been relatively mild, similar to a normal flu: headaches, a stuffy nose, a sore throat and muscle pains. She’s spent most of the past week resting in bed and taking baths to soothe her body aches. While taking care of Baldwin, her husband has also contracted the virus and is experiencing severe body aches as well.
In addition to her disappointment that the hypnobirthing and breastfeeding classes she had signed up for are canceled, her time in quarantine is now filled with anxious questions about how the disease may impact her baby.
Will the stress of this experience damage her baby neurologically? Will her baby be born early? Will she have to deliver by cesarean section to relieve pressure on her body and lungs, like so many stories she had read? Will she have to be secluded from her baby for days or weeks after birth? And what if her own symptoms worsen?
“This is our first baby, and it was so planned and wanted,” she said. “But had we known this awful thing would happen, would we have tried when we did?”
ProPublica is a nonprofit newsroom that investigates abuses of power. Sign up to receive our biggest stories as soon as they’re published.
The Transportation Security Administration ignored guidance from the Department of Homeland Security and internal pushback from two agency officials when it stockpiled more than 1.3 million N95 respirator masks instead of donating them to hospitals, internal records and interviews show.
Internal concerns were raised in early April, when COVID-19 cases were growing by the thousands and hospitals in some parts of the country were overrun and desperate for supplies. The agency held on to the cache of life-saving masks even as the number of people coming through U.S. airports dropped by 95% and the TSA instructed many employees to stay home to avoid being infected. Meanwhile, other federal agencies, including the Department of Veterans Affairs’ vast network of hospitals, scrounged for the personal protective equipment that doctors and nurses are dying without.
“We don’t need them. People who are in an infectious environment need them. Nobody is flying,” Charles Kielkopf, a TSA attorney based in Columbus, Ohio, told ProPublica. “You don’t take things for yourself. It’s the wrong thing to do.”
Kielkopf shared a copy of an official whistleblower complaint he filed Monday. In it, he alleges the agency had engaged in gross mismanagement that represented a “substantial and specific danger to public health.”
TSA has not required its screeners to wear N95s, which require fitting and training to use properly, and internal memos show most are using surgical masks, which are more widely available but are less effective and lack the same filtering ability.
Kielkopf raised a red flag last month about the TSA’s plan to store N95 respirators it had been given by Customs and Border Protection, which found more than a million old but usable masks in an Indiana warehouse. Both agencies are overseen by DHS. That shipment added to 116,000 N95s the TSA had left over from the swine flu pandemic of 2009, a TSA memo shows. While both stockpiles were older than the manufacturer’s recommended shelf life, the Centers for Disease Control and Prevention said that expired masks remain effective against spreading the virus.
Kielkopf and another TSA official in Minnesota suggested that the agency send its N95 masks to hospitals in early April, records show. Instead, TSA quietly stored many of them in its warehouse near the Dallas-Fort Worth airport and dispersed the rest to empty airports across the nation.
“We need to reserve medical masks for health care workers,” Kielkopf said, “not TSA workers who are behind an X-ray machine.”
The Number of Travelers Passing TSA Checkpoints Has Dropped to Historic Lows
Source: Transportation Security Administration
The TSA didn’t provide answers to several detailed questions sent by ProPublica, but spokesman Mark Howell said in an email that the agency’s “highest priority is to ensure the health, safety and security of our workforce and the American people.”
“With the support of CBP and DHS, in April, TSA was able to ensure a sufficient supply of N95 masks would be available for any officer who chose to wear one and completed the requisite training,” the statement read.
“We are continuing to acquire additional personal protective equipment for our employees to ensure both their and the traveling public’s health and safety based on our current staffing needs, and as supplies become available,” TSA said.
A review of federal contracting data shows the agency has mostly made modest purchases such as a $231,000 purchase for gallons of disinfectant, but has not reported any new purchases of N95s.
An internal TSA memo last month said the surplus of N95s was expected to last the agency about 30 days, but the same memo noted that estimate did not account for the drastic decline in security officers working at airports. ProPublica asked how long the masks were actually going to last, accounting for the decreased staffing levels.
“While we cannot provide details on staffing, passenger throughput and corresponding operations have certainly decreased,” the TSA statement said.
The trade journal Government Executive reported this week that internal TSA records showed most employee schedules have been “sharply abbreviated,” while an additional 8,000 security screeners are on paid leave over concerns that they could be exposed to the virus.
More than 500 TSA employees have tested positive for COVID-19, the agency reported, and five have died.
The CDC has not recommended the use of N95s by TSA staff, records show, but that doesn’t mean workers who have or want to wear them can’t.
In one April 7 email, DHS Deputy Under Secretary for Management Randolph D. Alles sent guidance to TSA officials, urging them to wear homemade cloth face coverings and maintain social distancing. But the N95s, which block 95% of particles that can transmit the virus, were in notoriously short supply and should be “reserved” for health care workers.
“The CDC has given us very good information about how to make masks that are suitable, so that we can continue to reserve medical masks and PPE for healthcare workers battling the COVID-19 pandemic,” Alles wrote.
But two days later, on April 9, Cliff Van Leuven, TSA’s federal security director in Minnesota, followed up and asked why he had been sent thousands of masks despite that guidance.
“I just received 9,000 N-95 masks that I have very little to no need for,” he said in the email, which was first reported by Government Executive. “We’ve made N95s available to our staff and, of the officers who wear masks, they overwhelmingly prefer the surgical masks we just received after a couple months on back order.”
Minnesota Gov. Tim Walz had publicly asked that anyone who had PPE donate their surplus to the state’s Department of Health, Van Leuven said in the email to senior TSA staff.
“I’d like to donate the bulk of our current stock of N-95s in support of that need and keep a small supply on hand,” he wrote, adding the Minneapolis-St. Paul International Airport had screened fewer than 1,500 people the previous day, about a third of which were airport staff.
Van Leuven declined to comment, referring questions to a TSA spokesperson.
Later that day, Kielkopf forwarded the concerns to TSA attorneys in other field offices, trying to get some attention to the stockpile he felt would be better used at hospitals.
“I am sharing with you some issues we are having with n95 masks in Minnesota,” he wrote. “And the tension between our increasing supply of n95 masks at our TSA airport locations and the dire need for them in the medical community.”
Weeks went by, and finally, on May 1, Kielkopf wrote: “I have been very disappointed in our position to keep tens of thousands of n95 masks while healthcare workers who have a medical requirement for the masks — because of their contact with infected people — still go without.”
DHS did not respond to ProPublica’s questions about why it transferred N95 masks to TSA despite a top official saying they should be reserved for healthcare workers.
“So now the TSA position is that we desperately need these masks for the protection of our people,” Kielkopf said. “At the same time, most of our people aren’t even working. It’s a complete 180 that doesn’t make any sense.”
ProPublica is a nonprofit newsroom that investigates abuses of power. Sign up to receive our biggest stories as soon as they’re published.
This story is co-published with PBS Frontline.
New York Attorney General Letitia James is looking into allegations that a Queens adult care facility has failed to protect residents from the deadly coronavirus and misled families about its spread, according to two lawmakers who asked for the inquiry and a relative of a resident who spoke to an investigator with the attorney general’s office.
In a separate action Tuesday, three residents of the Queens Adult Care Center sued the facility in federal court over similar allegations.
Both developments were prompted largely by ProPublica’s recent coverage of the facility, which houses both frail elderly residents and those with mental health issues. On April 2, we reported that workers and residents at the home were becoming ill with the coronavirus as residents wandered in and out of the home without any personal protective equipment. Family members later told ProPublica the management said no residents were sick with the virus at the time.
On April 25, ProPublica published a story and a short film with the PBS series Frontline about the harrowing experience of Natasha Roland, who rescued her father in the middle of the night as he suffered coronavirus symptoms so severe he could barely breathe. Roland, in heart-wrenching detail, described how the management of the Queens Adult Care Center repeatedly assured her that her 82-year-old father, Willie Roland, was safe, even as the virus swept through the facility. She said workers were too scared to care for him, forcing his girlfriend, Annetta King-Simpson, to do so. King-Simpson later fell ill herself. Roland and King-Simpson are now suing the facility in federal court.
Joe Singer and Katie Campbell/ProPublica
In an interview, Assemblywoman Catalina Cruz, whose district covers Corona, Elmhurst and Jackson Heights, said she was troubled by what ProPublica reported. She said she hoped the attorney general can determine whether the Queens Adult Care Center had broken any laws.
“It didn’t sit right with me. I thought something was off here. So I said let’s have the experts look at whether there was a crime or a civil violation,” she said. “Folks who live in this adult home deserve the same dignity as everyone else, and if their rights have been violated, someone needs to pay for that.”
Cruz said she had been suspicious of the facility for several years and had come across a community Facebook page where people posted complaints about treatment of residents at the center. When she saw the ProPublica stories, she said she decided to take action, along with City Council member Daniel Dromm, who had already written to the New York State Department of Health and the office of Gov. Andrew Cuomo about the spread of the coronavirus in the facility on several occasions.
“The plight of those living in adult care centers during this crisis was highlighted in a recent article published by ProPublica, which focused on the perils faced by the residents at the Queens Adult Day Care Center,” the lawmakers wrote in their April 27 letter to the attorney general and the governor’s office. “Failure to inform families about the health of loved ones, to lying and covering up deaths have become regular concerns we have received. We are aware that adult care centers are struggling to keep COVID-19 from affecting their residents and we also know that minorities have been disproportionately affected by the virus. It seems to us that management at this particular center have struggled to implement procedures and policies to protect the lives of its residents.”
Cruz said she received an update from the attorney general’s office on May 5, saying it was looking into the matter but would not provide specific details.
Days after the lawmakers sent the letter, Natasha Roland, 35, said she received a phone call from an investigator with the attorney general’s office. Roland said she recapped what she had previously told ProPublica: She began to worry about her father’s safety when nearby Elmhurst Hospital became a viral hot spot, but the management repeatedly told her there were no coronavirus cases in the facility. She said she only found out the truth weeks later when a worker she was friendly with advised her to come and pick up her father because the virus was raging through the facility and aides were becoming too scared to check on residents. In a subsequent interview, that worker denied telling Roland to pick up her dad.
A spokesperson for the attorney general would not confirm or deny a specific, active investigation into the Queens Adult Care Center, but said James has received hundreds of complaints related to COVID-19 inside nursing homes and adult care facilities across the state and is investigating many of them.
For its part, the Queens Adult Care Center has denied any wrongdoing and repeated its belief that Roland’s allegations are “baseless.”
“Sadly, select elected officials and ProPublica have been intentionally misled with baseless assertions and utter fabrications crafted by the daughter of one of our long-term residents,” said Hank Sheinkopf, a crisis communications spokesperson hired by the facility. “We have strong reason to believe that this individual is seeking to use her father and other select residents as pawns in an attempt to extort the facility. We are considering our legal options.”
He said the facility has “worked tirelessly” to protect its residents and is unaware of a “potential investigation,” but understood that “the AG’s office has contacted many nursing homes, adult care, and assisted living facilities seeking information. We are glad to be a resource to the AG’s office and have nothing to hide.”
Bruce Schoengood’s 61-year-old brother, Bryan, lives in the facility and shared a room with one of the first residents to become infected with COVID-19 and subsequently die of the disease. Bruce told ProPublica he only learned that his brother’s roommate had died by happenstance during a casual conversation with his brother, and that he has complained for more than a month about a lack of communication from the facility. He said he had not yet heard from anyone with the attorney general’s office but would welcome such a conversation.
In the meantime, Bryan Schoengood, Willie Roland and King-Simpson are suing the facility under the Americans with Disabilities Act. In a 59-page complaint, the group has asked a federal judge to appoint a special master to oversee the facility at the home’s expense to ensure that residents there are safe.
The lawsuit argues that residents have experienced a “gross failure to provide the most basic level of care to safeguard their health and safety in the context of a global health pandemic. People with disabilities are exposed to high risks of contracting the virus with no or few preventative measures in place. Residents who fall sick are left to languish in their room without proper access to medical care.”
The lawsuit claims that because the facility has failed to follow state and federal guidelines, “COVID-19 is rampant in the facility among residents and staff alike.”
Alan Fuchsberg is the Manhattan-based personal injury and civil rights attorney representing the three Queens Adult Care Center residents.
In an interview, he said that the facility may not have the resources to properly follow the guidelines, which is why a special master should be assigned to work with a team of outside experts to make sure it can.
“Right now the residents are in a tinderbox,” he said. “And if you drop a match in there, all hell breaks loose. It should be run right. We don’t need dozens of people dying in all our nursing homes and adult care facilities. Some are running better than others and QACC sounds like a place that is not run up to standards.”
He and Bruce Schoengood pointed out that they are not currently suing for damages, but rather to persuade a court to immediately intervene and offer support to the facility’s roughly 350 residents.
Schoengood said the goals of the lawsuit are twofold.
“I think it is both short term and long term,” he said. “Immediate intervention to put proper protocols in place to treat the sick and stop the spread of coronavirus and to communicate with family members. And in the long term I would like to see this facility much better prepared to handle another pandemic or a second wave.”
Responding to the charges in the lawsuit, Sheinkopf again said that “the allegations are baseless and utter fabrications. Queens Adult Care Center (QACC) continues to meet all state issued guidelines.”
ProPublica is a nonprofit newsroom that investigates abuses of power. Sign up to receive our biggest stories as soon as they’re published.
The links to the viral video “Plandemic” started showing up in my Facebook feed Wednesday. “Very interesting,” one of my friends wrote about it. I saw several subsequent posts about it, and then my brother texted me, “Got a sec?”
My brother is a pastor in Colorado and had someone he respects urge him to watch “Plandemic,” a 26-minute video that promises to reveal the “hidden agenda” behind the COVID-19 pandemic. I called him and he shared his concern: People seem to be taking the conspiracy theories presented in “Plandemic” seriously. He wondered if I could write something up that he could pass along to them, to help people distinguish between sound reporting and conspiracy thinking or propaganda.
So I watched “Plandemic.” I did not find it credible, as I will explain below. YouTube, Facebook and Vimeo have since removed it from their platforms for violating their guidelines. Now it’s available on its own site.
Sensational videos, memes, rants and more about COVID-19 are likely to keep coming. With society polarized and deep distrust of the media, the government and other institutions, such content is a way for bad actors to sow discord, mostly via social media. We saw it with Russia in the 2016 election and we should expect it to continue.
But what surprised me is how easily “Plandemic” sank its hooks into some of my friends. My brother also felt alarmed that his own church members and leaders in other churches might be tempted to buy into it.
The purpose of this column is not to skewer “Plandemic.” My goal is to offer some criteria for sifting through all the content we see every day, so we can tell the difference between fair reporting and something so biased it should not be taken seriously.
Here’s a checklist, some of which I shared with my friends on Facebook, to help interrogate any content — and that includes what we publish at ProPublica.
Is the Presentation One-Sided?
There’s never just one side to a story. I mentioned this point in 2018 when I wrote about my faith and the biblical basis for investigative reporting. One of my favorite Proverbs says, “The first to state his case seems right until another comes and cross-examines him.” So a fair presentation should at least acknowledge opposing points of view.
I didn’t see this in “Plandemic,” so I called the filmmaker, Mikki Willis, who is also the film’s narrator, to ask him whether I had somehow missed the other side of the argument. I had not. “The other side of the argument plays 24/7 on every screen in every airport and on every phone and in every home,” Willis said. “The people are only seeing one side of the story all the time. This is the other side of the story. This is not a piece that’s intended to be perfectly balanced.”
I asked Willis if it was fair to call his film “propaganda,” which the Oxford dictionary defines as “information, especially of a biased or misleading nature, used to promote or publicize a particular political cause or point of view.”
He said he doesn’t feel there’s anything misleading in his film, but otherwise the definition fits. And based on that definition he feels 100% of news reporting is propaganda. “What isn’t propaganda these days?” he asked. “In that sense, what we’re doing is fighting fire with fire.”
Is There an Independent Pursuit of the Truth?
The star of “Plandemic,” medical researcher Judy Mikovits, is controversial. The magazine Science reports that it published and then retracted one of her papers in 2011. A search warrant provided to ProPublica by one of her former attorneys shows she was fired from her position at Whittemore Peterson Institute, a research center in Nevada, in September 2011. Then she allegedly stole notebooks and a laptop computer from the Institute, the search warrant said, leading to an arrest warrant for alleged possession of stolen property and unlawful taking of computer data. She was arrested on Nov. 18, 2011, but denied wrongdoing. The charges were dropped.
But “Plandemic” ignores or brushes past these facts and portrays her as an embattled whistleblower. “So you made a discovery that conflicted with the agreed-upon narrative?” Willis says to Mikovits, introducing her as a victim. “And for that, they did everything in their powers to destroy your life.”
A typical viewer is not going to know the details about Mikovits’ background. But as the primary source of controversial information being presented as fact, it’s worth an online search. The fact-checking site PolitiFact details her arrest and criminal charges. Clearly, there’s more to her story than what’s presented in “Plandemic.” That should give us pause when we assess its credibility.
Is There a Careful Adherence to the Facts?
In “Plandemic,” Willis asks Mikovits about her arrest: “What did they charge you with?”
“Nothing,” she replies. “I was held in jail, with no charges.”
Being charged with a crime is one of those concrete facts that we can check out. Science magazine reported Mikovits’ arrest and felony charge. I also found a civil lawsuit she filed against the Whittemore Peterson Institute in 2014 in the U.S. District Court for the Southern District of California. “Mikovits was arrested on criminal charges…” her complaint says in the case, which was eventually dismissed.
I asked Willis about the apparent discrepancy, where she said in his film that she wasn’t charged, when court documents show that she was charged. After my inquiry, he said he spoke to Mikovits and now feels it is clear that she meant that the charges were dropped.
I tracked down Mikovits and she said what she meant in the film is that there were no charges of any type of wrongdoing that would have led to her being charged with being a fugitive from justice. She admitted that all the controversy has been hard for her to sort out. “I’ve been confused for a decade,” she told me. She said she would try to be more clear in the future when she talks about the criminal charge: “I’ll try to learn to say it differently,” she said.
This underscores the importance of careful verification, and it distinguishes the craft of journalism from other forms of information sharing. People often speak imprecisely when they’re telling their stories. It’s our duty to nail down precisely what they do and do not mean, and verify it independently. If we don’t, we risk undermining their credibility and ours. That’s in part why we at ProPublica and many other journalists often link directly to our underlying source documents, so you can verify the information yourself.
Are Those Accused Allowed to Respond?
Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases, is one of the nation’s leaders in the response to the coronavirus. In “Plandemic,” Mikovits accuses Fauci of a cover-up and of paying off people who perpetrate fraud, among other things. PolitiFact found no evidence to support the allegations against Fauci.
Every time I write a story that accuses someone of wrongdoing I call them and urge them to explain the situation from their perspective. This is standard in mainstream journalism. Sometimes I’ve gone to extreme lengths to get comments from someone who will be portrayed unfavorably in my story — traveling to another state and showing up at their office and their home and leaving a note if they are not there to meet me. “Plandemic” doesn’t indicate whether the filmmakers reached out to Fauci for his version of the story. So I asked Willis about it. “We did not,” he told me.
Are All Sources Named and Cited, and if Not, Is the Reason Explained?
All sources should be identified, with their credentials, so viewers can verify their expertise or possible biases. If they can’t be for some reason, then that should be explained. “Plandemic” features unnamed people in medical scrubs, presented as doctors, saying they’re being wrongly pressured to add COVID-19 on people’s death certificates or are not being allowed to use the drug hydroxychloroquine to treat patients. But the speakers are not named, so we can’t really tell who they are, or even if they are doctors at all. That makes it impossible to tell if they are credible.
I asked Willis why he didn’t name those people. He told me he was in a hurry to release the 26-minute version of “Plandemic,” but the doctors will be named in the final version. “We should have done that,” he said.
Does the Work Claim Some Secret Knowledge?
“Plandemic” calls itself a documentary that reveals “the hidden agenda behind COVID-19.” We are in the midst of a global pandemic where few people in the world can figure out what is happening or the right way to respond, let alone agendas. We have almost every journalist in the country writing about this. And if the truth about a conspiracy is out there, many people have an incentive to share it. But “Plandemic” would like us to think it’s presenting some exclusive bit of secret knowledge that is going to get at the real story. That’s not likely.
Plus, to be honest, there were so many conspiratorial details stacked on top of each other in the film I couldn’t keep them straight. When I spoke to Willis I told him I was having a hard time understanding his point. Then I took a stab at what I thought was the main thrust of his argument. “Are you saying that powerful people planned the pandemic and made it happen so they could get rich by making everyone get vaccines?” I asked.
It turns out Willis isn’t sure either. “We’re in the exploratory phase,” he told me. “I don’t know, to be clear, if it’s an intentional or naturally occurring situation. I have no idea.”
Then he went on to say that the pandemic is being politicized and used to take away our civil liberties and leverage other political policies. “Certain forces” have latched onto the situation, he said. “It’s too fishy.”
He had me at, “I have no idea.” That sums it up. This is a vast pandemic and massive catastrophe. Our country wasn’t prepared for it, and the response by our top leaders has been disjointed. We’re restricted to our homes. Many people have lost their jobs and some are afraid or sick or dying. That makes us vulnerable to exploitation by people who will present inaccurate or intellectually dishonest information that promises to tell us the truth.
Perhaps “Plandemic” is guilty of sloppy storytelling, or maybe people really do believe the things they’re saying in the video. Or perhaps they’re being intentionally dishonest, or it’s a biased connecting of the dots rooted in personal and professional grievances. I don’t know because I can’t get inside their heads to judge their motives.
Ultimately, we’re all going to need to be more savvy consumers when it comes to information, no matter how slickly it’s presented. This may be but a signal of what’s to come in the run-up to the 2020 presidential election, when memes and ads of unknown origin come across our social media feeds. There are standards for judging the credibility of the media we take in every day, so let’s apply them.
By regulatoryrx.blogspot.com
Published On :: Mon, 13 Jan 2020 18:26:00 +0000
PhillyCooke Consulting has added new services from the humble start more than five years ago, when I used to joke that the company included both me and my laptop.
In addition to continuing to provide regulatory consulting services, PhillyCooke Consulting now offers:
Submission Preparation Services for Ad Agencies
Medical Editing
Proofreading, and
Medical Writing.
You can learn a bit more about the expanded services here, or simply complete the "Contact Form" to request a free initial consultation.
Also, having completed law school (and been admitted to the bar in Pennsylvania), I am now able to offer legal services; however, the law practice is distinct from PhillyCooke Consulting. If you are interested in legal services related to the advertising and promotion of FDA-regulated products, please see FDAadLaw.com, which is a sister corporation to PhillyCooke Consulting.
Although the website is currently a bit spartan, the services offered are robust and address all aspects of advertising FDA-regulated products, including concerns related to the Lanham Act, privacy, and FDCA issues.
By regulatoryrx.blogspot.com
Published On :: Mon, 03 Feb 2020 14:54:00 +0000
UPDATE: The guidance mentioned below was released. Here's the link.
The FDA has released the CDER Guidance Agenda. For ad-promo professionals, the most most significant item is the inclusion of an item labeled:
Promotional Labeling and Advertising Considerations for Prescription Biological Reference and Biosimilar Products--Questions and Answers
Also notable is that no other advertising or promotional guidances are listed. The draft guidance on presenting risk information turned 10 years old last year. It seemed ripe for an update and perhaps even finalization. That seemed even more likely in the context of OPDP's study of the so-called one-click rule. That study was first announced in 2017. There's no update on the FDA website about the study, but I expected it to be completed last year.
FDA's social science research has clearly been influencing recent guidances, so I assumed (and continue to assume) that FDA would want to update the risk presentation guidance in light of its most recent research about presenting risks, including the one-click study. Apparently, we'll have to keep waiting.
BTW, for those interested in the topic of biosimilar promotion, the Drug Information Association's Advertising & Promotion Regulatory Affairs Conference will have a session covering this topic. Full disclosure: I sit on the programming committee for the conference and will be leading the medical device primer the day before the full conference kicks off.
Care home pharmacists redeployed, despite COVID-19 palliative care increase
By feeds.pjonline.com
Published On :: Fri, 24 Apr 2020 10:22 GMT
Exclusive: Pharmacy staff in care homes are being redeployed to cover other roles during the COVID-19 pandemic, even though demands on care homes are increasing rapidly, The Pharmaceutical Journal has learnt.
Pharmacy staff who have died during COVID-19 pandemic to be remembered during minute's silence
By feeds.pjonline.com
Published On :: Tue, 28 Apr 2020 09:49 GMT
Pharmacy staff who are thought to have died as a result of the COVID-19 pandemic are to be among the healthcare workers remembered with a minute’s silence on 28 April 2020.
Pharmacists will not be automatically included in government COVID-19 life assurance scheme
By feeds.pjonline.com
Published On :: Tue, 28 Apr 2020 16:21 GMT
Pharmacists will not be automatically eligible for a new government life assurance scheme for healthcare workers in England who die from COVID-19 during the pandemic.
Transcending boundaries: the role of pharmacists in gender identity services
By feeds.pjonline.com
Published On :: Thu, 30 Apr 2020 14:42 GMT
There has been a surge in demand for gender identity services in the UK over the past five years. Although the current role of pharmacists is limited, their potential contribution within a multidisciplinary team supporting transgender patients is beginning to emerge.
Community pharmacists will now be included in COVID-19 death-in-service scheme
By feeds.pjonline.com
Published On :: Thu, 30 Apr 2020 15:30 GMT
Community pharmacists are to be included in the government life assurance scheme for staff working on the frontline of the COVID-19 pandemic, the health secretary, Matt Hancock has announced.
Wholesalers 'almost completely out' of government-supplied PPE, trade body warns
By feeds.pjonline.com
Published On :: Fri, 1 May 2020 10:30 GMT
Wholesalers have “almost completely run out” of the personal protective equipment supplied by Public Health England for distribution to community pharmacies during the COVID-19 pandemic, the wholesaler trade body has warned.
Rising Leaders Conference Set for Nov. 18-19: Reserve Your Place Today!
By cohealthcom.org
Published On :: Thu, 12 Mar 2020 16:23:00 +0000
March 12, 2020 —[Note: Due to the coronavirus epidemic, the Conference has been rescheduled from May.] Healthcare was already the top issue for voters—and the coronavirus pandemic only intensifies the focus heading into a hotly-contested election. Both parties want to “do something” about the cost of healthcare and especially drug prices, and what happens when […]
FDA and FTC: Coronavirus Products Are Fraudulent, Could Delay Treatment
By cohealthcom.org
Published On :: Mon, 16 Mar 2020 19:02:11 +0000
March 16, 2020 – Amid rising concerns over “Novel Coronavirus Disease 2019” (COVID-19), the Food and Drug Administration and the Federal Trade Commission took action last week against seven companies for selling fraudulent COVID-19 products. The regulators sent Warning Letters to the companies because these products “are unapproved drugs that pose significant risks to patient […]
Despite Late Changes and COVID-19, CCPA Enforcement Date Remains July 1
By cohealthcom.org
Published On :: Mon, 20 Apr 2020 21:01:00 +0000
April 20, 2020 – With additional changes to the regulations still in administrative review and businesses grappling with pressing COVID-19 issues, a group of nearly 100 advertising trade associations, organizations and companies asked California Attorney General Xavier Becerra (D) to delay the July 1 enforcement date for the California Consumer Protection Act (CCPA). But it […]
COVID-19 Pandemic Likely to Affect FDA Product Approval Timelines
By cohealthcom.org
Published On :: Mon, 27 Apr 2020 17:50:36 +0000
April 27, 2020 – As the COVID-19 pandemic continues, the Food and Drug Administration (FDA) must balance safeguarding public health with the desire for timely product reviews. Staff members at the Center for Drug Evaluation and Research and the Center for Biologics Evaluation and Research are working diligently to keep all of these balls in […]
As COVID-19 Pandemic Continues, Promotion of Unapproved “Cures” Abounds
By cohealthcom.org
Published On :: Mon, 04 May 2020 20:17:45 +0000
May 4, 2020 – An important part of protecting the public health during the COVID-19 pandemic is making sure that the marketing of treatments or remedies that are not approved by the Food and Drug Administration (FDA) to treat the virus is stopped before consumers waste their money or potentially are harmed by these products. […]
EMA starts reviewing Gilead's remdesivir data to accelerate approval of COVID-19 antiviral
By www.fiercebiotech.com
Published On :: Fri, 01 May 2020 08:07:12 +0000
The European Medicines Agency has begun a rolling review of data on Gilead’s remdesivir, positioning it to cut the time it takes to decide whether to approve the drug in COVID-19 patients.
COVID-19 the focus, but Pfizer isn't ignoring other vaccine R&D as its pens new deal
By www.fiercebiotech.com
Published On :: Fri, 01 May 2020 08:47:53 +0000
Pfizer and partner BioNTech are right in the middle of one of the most important vaccine trials in the world right now, but that doesn’t mean the Big Pharma is taking its eyes off the inoculation ball elsewhere.
FDA delays decision on approval of Bristol Myers' CAR-T
By www.fiercebiotech.com
Published On :: Wed, 06 May 2020 12:02:53 +0000
The FDA has delayed its decision on whether to approve Bristol Myers Squibb’s CAR-T cell therapy by three months. Bristol Myers attributed the delay to its submission of additional information upon the request of the FDA.
Could Sanofi and Regeneron's Dupixent also treat age-related macular degeneration?
By www.fiercebiotech.com
Published On :: Thu, 07 May 2020 10:57:05 +0000
Sanofi and Regeneron’s Dupixent has become a popular treatment for atopic dermatitis and asthma. Now, a research team in Japan has discovered that IL-4 and its receptor—which Dupixent inhibits—could be promising targets for treating the eye disease age-related macular degeneration.
Moderna eyes 'early summer' start for phase 3 COVID-19 vaccine trial
By www.fiercebiotech.com
Published On :: Thu, 07 May 2020 12:10:49 +0000
Moderna is finalizing the protocol for a phase 3 trial of its COVID-19 vaccine with a view to starting the study early in the summer. The establishment of the timeline, which follows FDA clearance to run a phase 2 trial, puts Moderna on track to win approval for its mRNA vaccine mRNA-1273 next year.
{kind=link}
{kind=link}
{kind=link}
{kind=link}